Judicious alcohol consumption is a reasonable component of many successful ketogenic diets. But the practice can also be a dangerous minefield. Anne Mullins over at DietDoctor has a great article that will steer you away from the mines. An excerpt:
Nyström notes that alcohol is actually the fourth macronutrient after protein, fats and carbohydrates, and that in many nutrition studies its intake is often overlooked. In Mediterranean countries like Greece and Italy, alcohol makes up about 10 % of caloric intake and may partially contribute to the touted benefits of the Mediterranean diet, Nyström says.
Drinking alcohol, however, may slow weight loss for some. Dr. Sarah Hallberg advises her patients who are trying to lose weight and/or reverse diabetes to have a maximum 1 glass of wine for women and 2 for men, and not every day. “If they experience any weight stall, I recommend they stop the alcohol completely,” says Hallberg.
Both Dr. Jason Fung and Dr. Ted Naiman discourage any alcohol use among patients in their care who are still trying to lose weight, reverse diabetes or heal a fatty liver (see point 5). “I find alcohol is not conducive to steady weight loss,” says Fung.
Read the whole thing to learn about the dopamine reward system, alcohol abuse and addiction, liver diseases, and worse hangovers. If you regularly drink to the point of hangovers, that’s too much alcohol!
Steve Parker, M.D.
PS: Conquer Diabetes and Prediabetes includes a doctor-designed ketogenic diet as one option for weight loss and diabetes management.
Tomorrow is March 5th and it is five years since I began my personal health and weight recovery journey that I’ve dubbed “A Dietitian’s Journey“. While it began in 2017, in a way it still continues today and that is the point behind this post.
Five years ago, I was obese, had type 2 diabetes for the previous 8 years, and had developed dangerously high blood pressure.
Recommended. You’ll find out if low-carb eating put her diabetes into remission.
Judicious wine consumption is one component of the traditional healthy Mediterranean diet
Researchers compared three low-calorie diets and concluded that the Mediterranean option was the healthiest. The study at hand today is way too small to be considered anything but a pilot study. So results may not be replicable on a larger scale. I’d like to know how compliant study subjects were with the protocol, because 700 calories a day for six weeks is quite a challenge.
Comparison of short-term hypocaloric high-protein diets with a hypocaloric Mediterranean diet: Effect on body composition and health-related blood markers in overweight and sedentary young participants
Highlights
A hypocaloric Mediterranean diet provides all the necessary nutrients.
The hypocaloric Mediterranean diet reduces body mass and fat mass and maintains fat-free mass.
The hypocaloric Mediterranean diet is beneficial on metabolic and inflammation/muscle- damage indices.
Hypocaloric high-protein diets with and without whey supplementation reduce body mass and fat-free mass but not fat mass.
Hypocaloric high-protein diets with and without whey supplementation are adverse on metabolic and inflammation/muscle-damage indices
Abstract
Objectives
The aim of the present study was to compare the short-term effects of a hypocaloric Mediterranean diet and two high protein diets, with and without whey protein supplementation, on body composition, lipidemic profile, and inflammation and muscle-damage blood indices in overweight, sedentary, young participants.
Methods
Thirty-three young, overweight, male and female participants (mean ± SD age: 22.8 ± 4.8 y; body mass: 85.5 ± 10.2 kg; body fat percentage: 34.3% ± 8.1%) were randomly allocated to three different hypocaloric (−700 kcal/d) diets: a Mediterranean diet (MD; n = 10), a high-protein diet (HP; n = 10) diet, and a high-protein diet with whey supplementation (n = 10). The intervention lasted 6 wk. Body composition and biochemical indices were evaluated 1 wk before and after the nutritional interventions.
Results
Body and fat mass were decreased in the MD and HP groups (−3.5% ± 1.1% and −5.9% ± 4.2% for body and fat mass respectively in MD, and −1.7% ± 1.2% and −2.0% ± 1.8% for body and fat mass respectively in HP;P < 0.05), with no significant decline of fat-free mass observed in the MD group. The MD group’s diet beneficially altered the lipid profile (P < 0.05), but the HP and HPW groups’ diets did not induce significant changes. Subclinical inflammation and muscle-damage indices significantly increased in the HP and HPW groups (7.4% ± 3.5% and 66.6% ± 40.1% for neutrophils and CRP respectively in HP, and 14.3% ± 6.4% and 266.6% ± 55.1% for neutrophils and CRP respectively in HPW; P < 0.05) but decreased in the MD group (1.8% ± 1.2% and −33.3% ± 10.1% for neutrophils and CRP respectivelyc; P < 0.05). Energy intake of carbohydrates and proteins were significantly related to the changes in body composition and biochemical blood markers (r = −0.389 and −0.889; P < 0.05).
Conclusions
Among the three hypocaloric diets, only the Mediterranean diet induced positive changes in body composition and metabolic profile in overweight, sedentary individuals.
Steve Parker, M.D.
PS: I haven’t read the full report and don’t plan to any time soon.
Question Is cataract extraction associated with reduced risk of developing dementia?
Findings In this cohort study assessing 3038 adults 65 years of age or older with cataract enrolled in the Adult Changes in Thought study, participants who underwent cataract extraction had lower risk of developing dementia than those who did not have cataract surgery after controlling for numerous additional risks. In comparison, risk of dementia did not differ between participants who did or did not undergo glaucoma surgery, which does not restore vision.
Meaning This study suggests that cataract extraction is associated with lower risk [~30% less] of developing dementia among older adults.
Importance Visual function is important for older adults. Interventions to preserve vision, such as cataract extraction, may modify dementia risk.
Details in the abstract:
Objective To determine whether cataract extraction is associated with reduced risk of dementia among older adults.
Design, Setting, and Participants This prospective, longitudinal cohort study analyzed data from the Adult Changes in Thought study, an ongoing, population-based cohort of randomly selected, cognitively normal members of Kaiser Permanente Washington. Study participants were 65 years of age or older and dementia free at enrollment and were followed up biennially until incident dementia (all-cause, Alzheimer disease, or Alzheimer disease and related dementia). Only participants who had a diagnosis of cataract or glaucoma before enrollment or during follow-up were included in the analyses (ie, a total of 3038 participants). Data used in the analyses were collected from 1994 through September 30, 2018, and all data were analyzed from April 6, 2019, to September 15, 2021.
Exposures The primary exposure of interest was cataract extraction. Data on diagnosis of cataract or glaucoma and exposure to surgery were extracted from electronic medical records. Extensive lists of dementia-related risk factors and health-related variables were obtained from study visit data and electronic medical records.
Main Outcomes and Measures The primary outcome was dementia as defined by Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria. Multivariate Cox proportional hazards regression analyses were conducted with the primary outcome. To address potential healthy patient bias, weighted marginal structural models incorporating the probability of surgery were used and the association of dementia with glaucoma surgery, which does not restore vision, was evaluated.
Results In total, 3038 participants were included (mean [SD] age at first cataract diagnosis, 74.4 (6.2) years; 1800 women (59%) and 1238 men (41%); and 2752 (91%) self-reported White race). Based on 23 554 person-years of follow-up, cataract extraction was associated with significantly reduced risk (hazard ratio, 0.71; 95% CI, 0.62-0.83; P < .001) of dementia compared with participants without surgery after controlling for years of education, self-reported White race, and smoking history and stratifying by apolipoprotein E genotype, sex, and age group at cataract diagnosis. Similar results were obtained in marginal structural models after adjusting for an extensive list of potential confounders. Glaucoma surgery did not have a significant association with dementia risk (hazard ratio, 1.08; 95% CI, 0.75-1.56; P = .68). Similar results were found with the development of Alzheimer disease dementia.
Conclusions and Relevance This cohort study found that cataract extraction was significantly associated with lower risk of dementia development. If validated in future studies, cataract surgery may have clinical relevance in older adults at risk of developing dementia.
What else reduces risk of dementia? The Mediterranean Diet!
Semaglutide and liraglutide are drugs that were developed to treat diabetes and are FDA-approved for that. They are given by subcutaneous injection. Semaglutide is also FDA-approved for weight loss in non-diabetics if certain conditions are met.
Once-weekly semaglutide outperformed daily liraglutide in overweight and obese non-diabetics.
Question Among adults with overweight or obesity without diabetes, what is the effect of once-weekly subcutaneous semaglutide, 2.4 mg, vs once-daily subcutaneous liraglutide, 3.0 mg, on weight loss when each is added to counseling for diet and physical activity?
Findings In this randomized clinical trial that included 338 participants, mean body weight change from baseline to 68 weeks was –15.8% with semaglutide vs –6.4% with liraglutide, a statistically significant difference.
Meaning Among adults with overweight or obesity without diabetes, once-weekly subcutaneous semaglutide, compared with once-daily subcutaneous liraglutide, added to counseling for diet and physical activity resulted in significantly greater weight loss at 68 weeks.
For prevention or improvement of overweight- and obesity-related illnesses, aim for loss of at least 5 to 10% of body weight. Assuming you’re overweight or obese in the first place. 16% body weight change is significant. 16% of 300 pounds (136 kg) would be 48 pounds (22 kg).
Steve Parker, M.D.
PS: My book’s less expensive than those drugs. And no needles!
Stages of liver damage. Healthy, fatty, liver fibrosis and cirrhosis
About one quarter of the world’s adults have excess fat accumulation in the the liver called non-alcoholic fatty liver disease (NAFLD). This can lead to liver inflammation, scarring (cirrhosis), and liver cancer. The adverse effects of liver fat can be prevented by loss of that fat. The most common medical recommendation to accomplish that is to loss excess body weight via any reasonable method.
A study published in Gut last year found greater reduction in liver fat in those eating a “green-Mediterranean” diet compared to a regular Mediterranean diet over 18 months. Both diets were supplemented with walnuts 28 grams/day. Details of the green-Med diet:
In addition to [physical activity] and the provision of 28 g/day walnuts, the green-MED diet was restricted in processed and red meat and was richer in plants and polyphenols. The participants were guided to further consume the following provided items: 3–4 cups/day of green tea and 100 g/day of frozen Wolffia globosa (Mankai strain) plant frozen cubes, as a green shake replacing dinner. Both green tea and Mankai together provided additional daily intake of 800 mg polyphenols ((GAE), according to Phenol-Explorer and Eurofins lab analysis, including catechins (flavanols)) beyond the polyphenol content in the prescribed MED diet. Both the MED and green-MED diets were equally calorie-restricted (1500–1800 kcal/day for men and 1200–1400 kcal/day for women).
The researchers don’t tell us where to get frozen Wolffia globosa (Mankai strain) plant frozen cubes.
Study participants were almost all men, so results may not apply to women.
Viagra (one brand name for generic sildenafil) is used to treat erectile dysfunction and pulmonary hypertension. I bet that usage for ED is far more common than for pulmonary hypertension.
From an article published in Dec 2021 by National Institutes of Health:
…the team analyzed insurance claims data from more than 7 million Americans. They found that the people (mostly men) who took sildenafil were 69% less likely to develop AD [Alzheimer’s Disease] over 6 years than those who did not take the drug. This association between sildenafil and AD held after adjusting for sex, age, and other diseases and conditions.
To understand how sildenafil might affect AD, the researchers grew neurons from stem cells derived from AD patients. Exposing the cells to sildenafil led to increased growth of neurites, which connect neurons to each other, and decreased tau phosphorylation, an early biomarker of AD.
Taken together, these results show an association between sildenafil use and reduced AD risk. But the researchers emphasize that they haven’t shown that sildenafil prevents or reverses AD.
These things usually don’t pan out, but one can hope. How often were these guys taking viagra? Once a month? Twice a week? To treat erectile dysfunction, sildenafil is typically taken as needed one hour before sexual activity. A typical dose for pulmonary hypertension is 20 mg by mouth three times a day, every day. Would this drug affect dementia in women? As they say, further studies are needed.
…according to U.S. News & World Report. Click through if interested in the two runners-up. I think a low-carb version of Mediterranean is better for most folks.
Olives, olive oil, and vinegar: classic Mediterranean foods
I’m surprised they ranked Atkins as the “Best Fast Weight-Loss Diet.” Looks like we’re getting over our collective phobia about saturated fat. “Keto Diet” ranked #4 in that category.
The doses vary, depending on body weight, age, tolerance to the drug. Generally, the higher doses are for younger and heavier folks. If one gets plentiful sunlight exposure, the oral vitamin D may not be needed.
Other strategies during disease surges (or always?):
Regular exercise
Lose excess weight, especially if obese (BMI over 30)
Maintain normal blood sugars (if diabetic, keep HgbA1c under 6.5%)
Avoid close, prolonged contact with coughing and sneezing people, especially in enclosed spaces
Frequent hand-washing if exposed to public doorknobs, elevator buttons, or other potentially contaminated surfaces, or if around sick (coughing and/or sneezing) people
Avoid sick people who are coughing and sneezing
Eat healthful food
Did you notice I haven’t mentioned masks? I’m not a big believer. Do I wear an N-95 mask when I’m seeing a COVID-19 patient at the hospital? You bet. And the mask was fit-tested. Is that testing available to the general public? Not that I’m aware.
Do I have great data to support all these strategies? No, but some. Are they recommended by the CDC or NIH (Nat’l Institutes of Health)? I don’t know or care. I’ve lost faith in them. I’m afraid they’ve been bought and paid for by Big Pharma (and others?).
I don’t know about your personal health and medical history. I’m not your doctor. If you’re considering any of these recommendations, consult your personal physician before implementation.
The patient is wise to look away. If you watch the needle go in, it’ll hurt more.
I was motivated to write this post by the failures and risks of the rushed vaccines. Vaccination might be helpful if you are sickly, over 65, or have underlying conditions such as diabetes, active cancer, a poor immune system, obesity (especially BMI over 35), or some other co-morbidities. I see both very healthy, vigorous 65-year-olds, and sickly 65-year-olds. Which one are you? If you’re over 80, you may have nothing to lose by vaccinating. Average U.S. life expectancy is 79 years, less for men, longer for women.
“So, yes back to my thoughts on Omicron – please keep taking that vitamin D3 and get your levels tested, if you haven’t already. Use a formulation that combines the D3 with Vitamins A and K. Please keep up with the zinc, vitamin C and magnesium. Work on weight control, glycemic control and please exercise! All are important.”
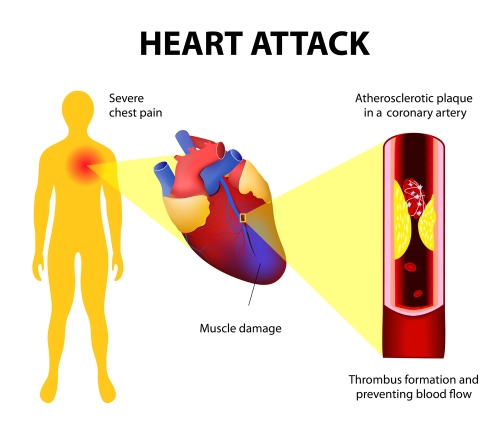
Heart attacks and chest pains are linked to blocked arteries in the heart (coronary artery disease)
What are ultra-processed foods? I’m not paying $35 for the scientific article to find out. If you can grab the definition from your copy, please share in the Comments section. The 2020 profit from my publishing company was only $937.08, so I’m watching my expenses.
Here’s the free abstract:
ABSTRACT
Background
Higher ultra-processed food intake has been linked with several cardiometabolic and cardiovascular diseases. However, prospective evidence from US populations remains scarce.
Objectives
To test the hypothesis that higher intake of ultra-processed foods is associated with higher risk of coronary artery disease.
Ultra-processed versus processed?
Methods
A total of 13,548 adults aged 45–65 y from the Atherosclerosis Risk in Communities study were included in the analytic sample. Dietary intake data were collected through a 66-item FFQ. Ultra-processed foods were defined using the NOVA classification, and the level of intake (servings/d) was calculated for each participant and divided into quartiles. We used Cox proportional hazards models and restricted cubic splines to assess the association between quartiles of ultra-processed food intake and incident coronary artery disease.
Results
There were 2006 incident coronary artery disease cases documented over a median follow-up of 27 y. Incidence rates were higher in the highest quartile of ultra-processed food intake (70.8 per 10,000 person-y; 95% CI: 65.1, 77.1) compared with the lowest quartile (59.3 per 10,000 person-y; 95% CI: 54.1, 65.0). Participants in the highest compared with lowest quartile of ultra-processed food intake had a 19% higher risk of coronary artery disease (HR: 1.19; 95% CI: 1.05, 1.35) after adjusting for sociodemographic factors and health behaviors. An approximately linear relation was observed between ultra-processed food intake and risk of coronary artery disease.Conclusions
Higher ultra-processed food intake was associated with a higher risk of coronary artery disease among middle-aged US adults. Further prospective studies are needed to confirm these findings and to investigate the mechanisms by which ultra-processed foods may affect health.
I admit I must eat some ultra-processed foods, but try to limit them.
Heart disease is the #1 killer in the developed world, even more lethal the COVID19! If you haven’t chosen your New Years’ weight-loss diet yet, consider one low in ultra-processed foods, like the Mediterranean diet.
Not ultra-processed. Salmon is a rich source of heart-healthy omega-3 fatty acids