

Stop reading this sciencey post when you get bored
According to Roy Taylor, “type 2 diabetes is a potentially reversible metabolic state precipitated by the single cause of chronic excess intraorgan fat.” The organs accumulating fat are the liver and pancreas. He is certain “…that the disease process can be halted with restoration of normal carbohydrate and fat metabolism.” I read Taylor’s article published earlier this year in Diabetes Care.
[Do you remember that report in 2011 touting cure of T2 diabetes with a very low calorie diet? Taylor was the leader. The study involved only 11 patients, eating 600 calories a day for eight weeks.]
Dr. Taylor (M.D.) says that severe calorie restriction is similar to the effect of bariatric surgery in curing or controlling diabetes. Within a week of either intervention, liver fat content is greatly reduced, liver insulin sensitivity returns, and fasting blood sugar levels can return to normal. During the first eight weeks after intervention, pancreatic fat content falls, with associated steadily increasing rates of insulin secretion by the pancreas beta cells.
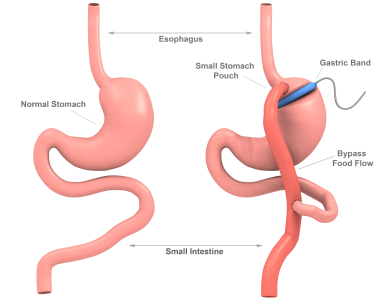
Band Gastric Bypass Surgery (not the only type of gastric bypass): very successful at “curing” T2 diabetes if you survive the operation
Taylor’s ideas, by the way, dovetail with Roger Unger’s 2008 lipocentric theory of diabetes. Click for more ideas on the cause of T2 diabetes.
Here are some scattered points from Taylors article. He backs up most of them with references:
- In T2 diabetes, improvement in fasting blood sugar reflects improved liver insulin sensitivity more than muscle insulin sensitivity.
- The more fat accumulation in the liver, the less it is sensitive to insulin. If a T2 is treated with insulin, the insulin dose is positively linked to how much fat is in the liver.
- In a T2 who starts insulin injections, liver fat stores tend to decrease. That’s because of suppression of the body’s own insulin delivery from the pancreas to the liver via the portal vein.
- Whether obese or not, those with higher circulating insulin levels “…have markedly increased rates of hepatic de novo lipogenesis.” That means their livers are making fat. That fat (triglycerides or triacylglycerol) will be either burned in the liver for energy (oxidized), pushed into the blood stream for use elsewhere, or stored in the liver. Fatty acids are components of triglycerides. Excessive fatty acid intermediaries in liver cells—diglycerides and ceramide—are thought to interfere with insulin’s action, i.e., contribute to insulin resistance in the liver.
- “Fasting plasma glucose concentration depends entirely on the fasting rate of hepatic [liver] glucose production and, hence, on its sensitivity to suppression by insulin.”
- Physical activity, low-calorie diets, and thiazolidinediones reduce the pancreas’ insulin output and reduce liver fat levels.
- Most T2 diabetics have above-average liver fat content. MRI scans are more accurate than ultrasound for finding it.
- T2 diabetics have on average only half of the pancreas beta cell mass of non-diabetics. As the years pass, more beta cells are lost. Is the a way to preserve these insulin-producing cells, or to increase their numbers? “…it is conceivable that removal of adverse factors could result in restoration of normal beta cell number, even late in the disease.”
- “Chronic exposure of [pancreatic] beta cells to triacylglycerol [triglycerides] or fatty acids…decreases beta cell capacity to respond to an acute increase in glucose levels.” In test tubes, fatty acids inhibit formation of new beta cells, an effect enhanced by increased glucose concentration.
- There’s a fair amount of overlap in pancreas fat content comparing T2 diabetics and non-diabetics. It may be that people with T2 diabetes are somehow more susceptible to adverse effects of the fat via genetic and epigenetic factors.
- “If a person has type 2 diabetes, there is more fat in the liver and pancreas than he or she an cope with.”
- Here’s Dr. Taylor’s Twin Cycle Hypothesis of Etiology of Type 2 Diabetes: “The accumulation of fat in liver and secondarily in the pancreas will lead to self-reinforcing cycles that interact to bring about type 2 diabetes. Fatty liver leads to impaired fasting glucose metabolism and increases export of VLDL triacylglcerol [triglycerides], which increases fat delivery to all tissues, including the [pancreas] islets. The liver and pancreas cycles drive onward after diagnosis with steadily decreasing beta cell function. However, of note, observations of the reversal of type 2 diabetes confirm that if the primary influence of positive calorie balance is removed, the the processes are reversible.”
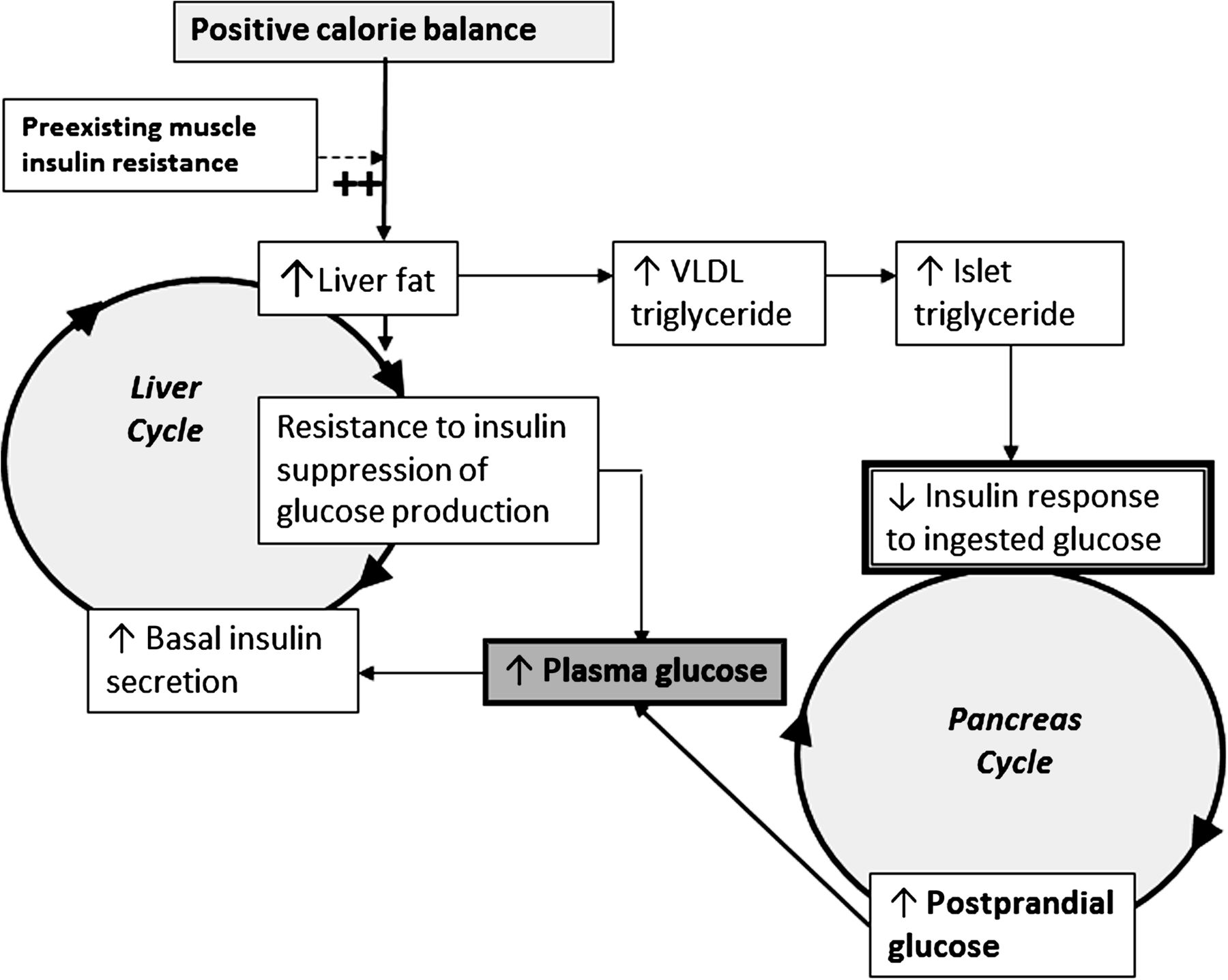
Figure 6 from the article: Dr. Taylor’s Twin Cycle Hypothesis of Etiology of Type 2 Diabetes
- The caption with Figure 6 states: “During long-term intake of more calories than are expended each day, any excess carbohydrate must undergo de novo lipogenesis [creation of fat], which particularly promotes fat accumulation in the liver.”
- “The extent of weight gloss required to reverse type 2 diabetes is much greater than conventionally advised.” We’re looking at around 15 kg (33 lb) or 20% of body weight, assuming the patient is obese to start. “The initial major loss of body weight demands a substantial reduction in energy intake. After weight loss, steady weight is most effectively achieved by a combination of dietary restriction and physical activity.”
Dr. Taylor doesn’t specify how much calorie restriction he recommends, but reading between the lines, I think he likes his 600 cals/day for eight weeks program. That will have a have a high drop-out rate. I suspect a variety of existing ketogenic diets may be just as successful and more realistic, even if it takes more than eight weeks. I wonder how many of the 11 “cures” from the 2011 study have persisted.
Reference: Taylor, Roy. Type 2 diabetes: Etiology and reversibility. Diabetes Care, April 2013, vol. 36, no. 4, pp:1047-1055.
Update December 16, 2013:
Some wild and crazy guys tried this method at home. Click for results.
h/t commenter PhilT.



