An up-and-coming theory to explain type 2 diabetes suggests that abnormal lipid metabolism, not glucose/sugar metabolism, is the primary metabolic defect. Roger H. Unger, M.D., writes about this in the March 12, 2008, issue of the Journal of the American Medical Association.
Early in the writing of this blog entry, I realized it is much too technical for many readers. I’m writing this to solidify my own understanding of a new theory. If you are not interested in physiology, you can quit reading now.
Still with me?
Definitions and Physiology
Diabetes is defined by high blood glucose (sugar) levels.
The lipid family includes triglycerides (fats and oils), sterols (e.g., cholesterol), and phospholipids (e.g., lecithin, a major cell membrane component). Fats are almost entirely composed of trigylcerides. When fats are broken down, fatty acids are produced. On the other hand, fatty acids can be joined together, along with glycerol, to form triglycerides.
Glycogen is a storage form of glucose in liver and muscle tissue.
Insulin is a protein hormone produced by pancreatic beta cells. Insulin:
-
lowers blood glucose levels by driving glucose into cells
-
inhibits breakdown of glycogen into glucose
-
inhibits formation of new glucose molecules by the body
-
stimulates glycogen formation
-
promotes storage of triglycerides in fat cells (i.e., lipogenesis, fat accumulation)
-
promotes formation of fatty acids (triglyceride building blocks) by the liver
-
inhibits breakdown of stored triglycerides
-
supports protein synthesis.
Fatty acids in muscle tissue block the uptake of glucose from the bloodstream by muscle cells. Fatty acids in liver tissue impair the ability of insulin to suppress breakdown of glycogen into glucose, and impair the ability of insulin to suppress production of new glucose molecules. In other words, an “excessive fatty acid” environment in liver and muscle tissue promotes elevated glucose levels.
Got that? [This is very difficult material.] Now on to . . .
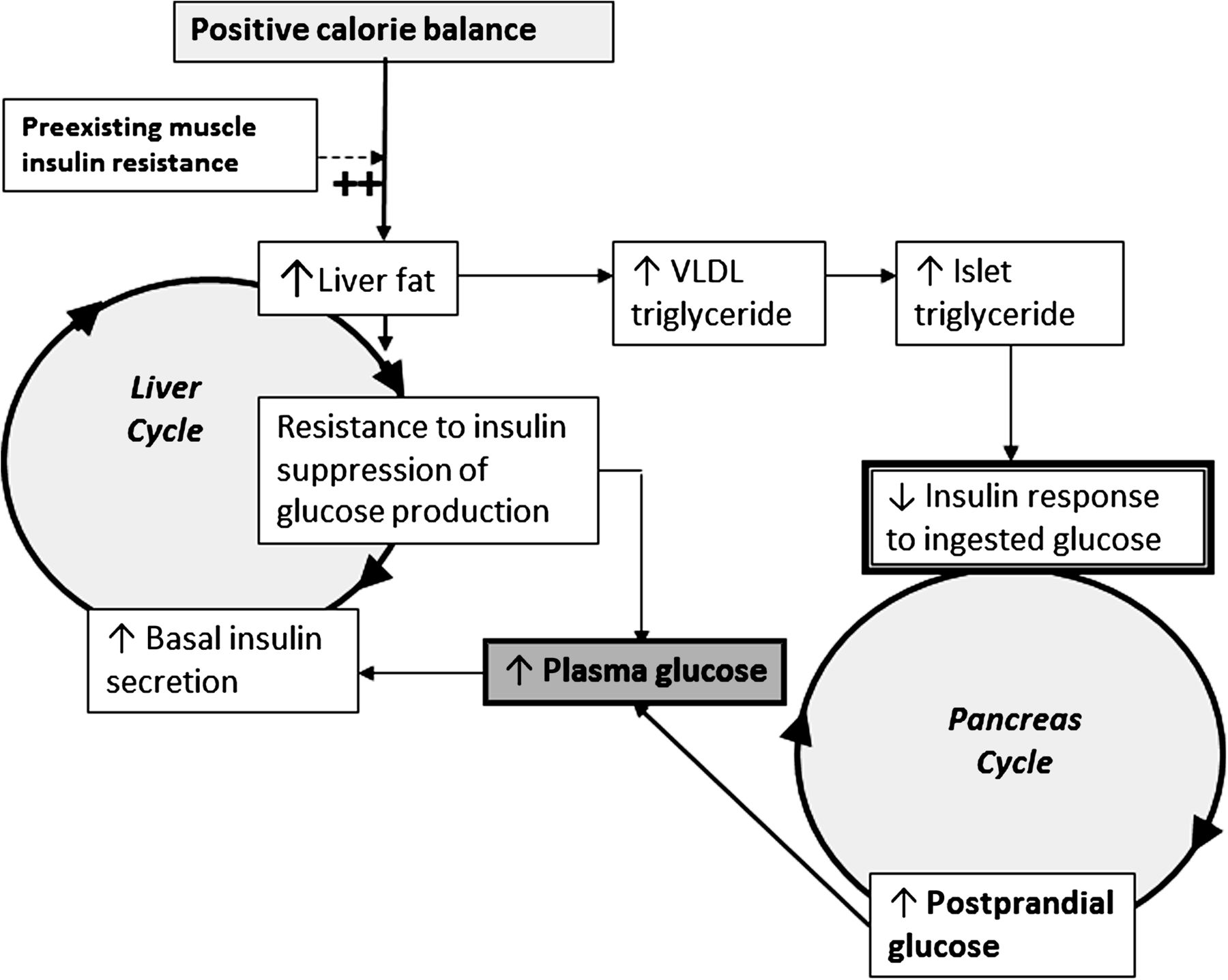
The Lipocentric Theory of Type 2 Diabetes
Type 2 diabetes may be caused by:
- Eating too many calories, leading to…
- High insulin levels, leading to…
- Stimulation of fat production, leading to…
- Increased body fat, leading to…
- Deposition of lipids in cells where they don’t belong (that is, not in fat cells), leading to…
- Resistance to insulin’s effects on glucose metabolism, leading to…
- Lipid accumulation in pancreatic beta cells, damaging them, leading to…
- Elevated blood glucose levels, i.e., diabetes.
Perhaps the key to understanding this is to know that “insulin resistance” refers to insulin having less ability to suppress glucose production by the liver, or less ability of various tissues to soak up circulating glucose. Insulin resistance thereby leads to elevated glucose levels. But insulin’s effect of “producing fats” (lipogenesis) continues unabated. Excessive fats, actually fatty acids, accumulate not only in fat cells, but also in liver cells, muscle cells, pancreatic beta cells, and others. This lipid overload can damage those cells.
If This Theory Is Correct, So What?
Steps #1 and 2 of the lipocentric theory involve excessive caloric intake and high circulating insulin levels, leading to problems down the road. So overweight people should restrict calories and try to lose at least a modest amount of weight. Particularly if already having type 2 diabetes or prone to it.
And what about people with type 2 diabetes who have insulin resistance and have poorly controlled glucose levels? Most of these have high insulin levels already, contributing to a fat-producing state. Adding more insulin, by injection, would not seem to make much sense. The extra insulin would bring glucose levels down, but might also cause lipid overload with associated cellular damage. Effective clinical strategies according to Dr. Unger would include 1) caloric restriction, which helps reduce weight, high insulin levels, and fat production, and 2) if #1 fails, add anti-diabetic drugs that reduce caloric intake (exenatide?), that reduce lipid overload (which drug?), or that do both. Dr. Unger suggests consideration of bariatric surgery, for caloric restriction and cure of diabetes.
Compared with dietary fats and proteins, carbohydrates generally cause higher circulating insulin levels. And type 2 diabetics taking insulin shots need higher doses for higher intakes of carbohydrate. So it makes sense to me to consider preferential reduction of carbohydrate intake if someone is going to reduce caloric intake.
Dr. Unger and I agree that reduction of excessive food intake and excess body fat is critically important for overweight people with type 2 diabetes.
Steve Parker, M.D.
References: Unger, Roger H. Reinventing Type 2 Diabetes: Pathogenesis, Treatment, and Prevention. Journal of the American Medical Association, 299 (2008): 1185-1187.