Whether you are traveling and can’t cook or you are celebrating something special with people you love, Olive Garden has some low-carb options that are simply delicious!
They might be known for their endless breadsticks and overflowing plates of pasta, but there are some keto-friendly choices on the menu, too. You just have to know where to look.
Olive Garden is also known for its large portions, so you will have to think ahead before eating everything on your plate.
When you don’t have time to cook or just want to dine out, Olive Garden can be an appealing option for people on a ketogenic diet. Thankfully, there are ways to eat a keto meal at Olive Garden – you just have to be a little creative with a custom order!
Thank you, Lisa.
Steve Parker, M.D.
PS: Conquer Diabetes and Prediabetes includes a ketogenic option.
Not sure if this is chicken or tuna salad with walnuts and grapes
Periodically there are outbreaks of illness caused by eating contaminated leafy greens. The contaminants are usually bacteria such as E coli and Salmonella. The illness is typically diarrhea, sometimes with belly cramps, nausea, and vomiting. And rare deaths.
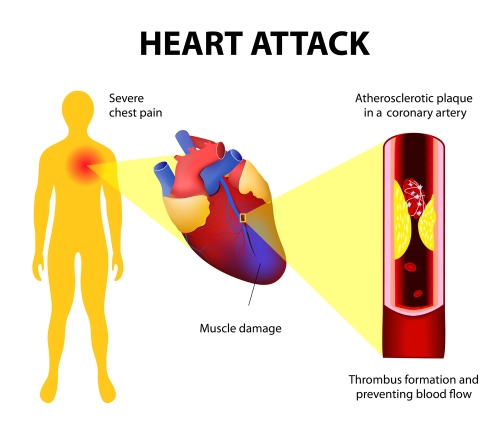
Heart attacks and chest pains are linked to blocked arteries in the heart
We’re all gonna die of something.
The #1 cause of death in the U.S. is coronary artery disease (CAD), which causes heart attacks, sudden cardiac death, and some cases of congestive heart failure. Folks with diabetes have a higher-than-average risk of CAD. Blockage in the heart arteries typically develops over years and many people are walking around not knowing it’s there. The lucky ones develop warning signs like transient chest pain or shortness of breath on exertion. After consulting a physician, the next step may be a “stress test” or some sort or imaging of the arteries of the heart.
Angiography refers to imaging of arteries or veins. Angiography of the heart arteries is helpful in diagnosing blockage of arteries that may cause heart attacks or sudden cardiac death in the future.
CT stands for computerized tomography: x-rays obtain images that are then manipulated by computer technology to provide more information than plain x-ray technology alone. CT angiography of the heart arteries is done with iodinated contrast injected into the low-pressure venous system of circulation. In contrast, standard arterial angiography involves introduction of a needle (and catheter) into the high-pressure arterial system, usually the femoral artery in the groin or the smaller radial artery in the wrist. Standard arterial angiography is associated with a higher risk of complications such as leakage of blood from the artery. Another potential complication is embolization of arterial plaque or clots downstream from the arterial puncture. Because of the higher complication rate in the arterial system, standard angiography is considered “invasive.”
Among patients referred for invasive coronary angiography (ICA) because of stable chest pain and intermediate pretest probability of coronary artery disease, the risk of major adverse cardiovascular events was similar in the CT group and the ICA group. The frequency of major procedure-related complications was lower with an initial CT strategy.
I bet the non-invasive CT is also less expensive than standard arterial angiography.
Steve Parker, M.D.
PS: You now what else help prevent heart attacks and cardiac death? The Mediterranean diet.
From the U.S. Food and Drug Administration May 13, 2022:
Today, the U.S. Food and Drug Administration approved Mounjaro (tirzepatide) injection to improve blood sugar control in adults with type 2 diabetes, as an addition to diet and exercise. Mounjaro was effective at improving blood sugar and was more effective than the other diabetes therapies with which it was compared in clinical studies.
“Given the challenges many patients experience in achieving their target blood sugar goals, today’s approval of Mounjaro is an important advance in the treatment of type 2 diabetes,” said Patrick Archdeacon, M.D., associate director of the Division of Diabetes, Lipid Disorders, and Obesity in the FDA’s Center for Drug Evaluation and Research.
Type 2 diabetes, the most common form of diabetes, is a chronic and progressive condition in which the body does not make or use insulin normally, leading to high levels of glucose (sugar) in the blood. More than 30 million Americans have type 2 diabetes. Despite the availability of many medications to treat diabetes, many patients do not achieve the recommended blood sugar goals.
Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are hormones involved in blood sugar control. Mounjaro is a first-in-class medicine that activates both the GLP-1 and GIP receptors, which leads to improved blood sugar control. Mounjaro is administered by injection under the skin once weekly, with the dose adjusted as tolerated to meet blood sugar goals.
Three different doses of Mounjaro (5 milligrams, 10 milligrams and 15 milligrams) were evaluated in five clinical trials as either a stand-alone therapy or as an add-on to other diabetes medicines. The efficacy of Mounjaro was compared to placebo, a GLP-1 receptor agonist (semaglutide) and two long-acting insulin analogs.
On average, patients randomized to receive the maximum recommended dose of Mounjaro (15 milligrams) had lowering of their hemoglobin A1c (HbA1c) level (a measure of blood sugar control) by 1.6% more than placebo when used as stand-alone therapy, and 1.5% more than placebo when used in combination with a long-acting insulin. In trials comparing Mounjaro to other diabetes medications, patients who received the maximum recommended dose of Mounjaro had lowering of their HbA1c by 0.5% more than semaglutide, 0.9% more than insulin degludec and 1.0% more than insulin glargine.
Obesity was common among study participants, with an average body mass index of 32 to 34 kilograms/height in meters squared reported at the time of enrollment. Among patients randomized to the maximum recommended dose, the average weight loss with Mounjaro was 15 pounds more than placebo when neither were used with insulin and 23 pounds more than placebo when both were used with insulin. The average weight loss with the maximum recommended dose of Mounjaro was 12 pounds more than semaglutide, 29 pounds more than insulin degludec and 27 pounds more than insulin glargine. Those patients receiving insulin without Mounjaro tended to gain weight during the study.
Mounjaro can cause nausea, vomiting, diarrhea, decreased appetite, constipation, upper abdominal discomfort and abdominal pain.
Mounjaro causes thyroid C-cell tumors in rats. It is unknown whether Mounjaro causes such tumors, including medullary thyroid cancer, in humans. Mounjaro should not be used in patients with a personal or family history of medullary thyroid cancer or in patients with Multiple Endocrine Neoplasia syndrome type 2.
Mounjaro has not been studied in patients with a history of pancreas inflammation (pancreatitis), and it is not indicated for use in patients with type 1 diabetes.
Mounjaro received priority review designation for this indication. A priority review designation directs overall attention and resources to the evaluation of applications for drugs that, if approved, would be significant improvements in the safety or effectiveness of the treatment, diagnosis or prevention of serious conditions.
The starting dose is 2.5 mg subcutaneously once weekly. After four weeks dose can be increased to 5 mg once weekly. Dose can be increased every four weeks to a maximum of 15 mg once weekly.
Study participants were enrolled from Nov 2020 to Feb 2021. So probably before the delta and omicron variants. Outpatients were assigned either to a “standard program” of home monitoring or the standard program + pulse oximetry. There was no difference between groups in terms of “number of days alive and out of the hospital.” For the 30-day trial, that number was 29.4-29.5. In other words, very few of the ~1000 enrolees got very sick.
Pulse oximeters are readily available in the U.S. for ~$40.
The standard program was “COVID Watch, a 2-week program involving twice-daily automated text messages inquiring about dyspnea and offering rapid callbacks from nurses when appropriate. This program has been associated with improved survival as compared with no remote monitoring.5“
I spent about 10 mins trying to find the age of these patients. No luck. I don’t even now if they were adults. Thanks, NEJM. I’m not totally convinced that outpatient oximetry has no role in home treatment of COVID-19. But clearly not every patient needs it. Perhaps just those at high risk of hospitalization and death.
Steve Parker, M.D.
PS: Obesity is a risk factor for severe disease from COVID-19. Let me help you do something about it.
If image owner (who?) objects to me posting the image, let me know and I’ll delete it.
This looks and sounds intriguing but I haven’t tried it yet. I’ve never combined avocado and salmon in an entree. I never imagined I’d like avocado in chicken soup, but it’s become a Parker Compound favorite.
The study at hand was very small, only 20 participants. So results may not be reproducible. The Canadian researchers’ main conclusion: “This is the longest duration MCT Alzheimer Disease study to date. Eighty percent had stabilization or improvement in cognition, and better response with 9‐month continual MCT oil.”
MCT stands for medium chain triglycerides, which apparently are derived from coconut and palm oil. The MCTs provide a source of energy for the brain – ketones – as a partial substitute for the brain’s usual energy source, glucose.
Study participants as expected were elderly and had mild to moderate Alzheimer Disease. Folks with diabetes were excluded from participation.
The article introduction has some interesting facts:
The brain is an obligate glucose metabolizer using 120 to 130 g/day of glucose. It uses 16% of the body’s total O2 consumption, despite representing only 2.0% to 2.3% of adult body weight. In conditions of low carbohydrate intake or fasting, the body uses ketones (acetoacetate and beta hydroxybutyrate [BHB]) as an alternative energy source to glucose. Ketones are normally generated in fasting states from beta‐oxidation of adipose stores to maintain cerebral function. In long‐term fasting, ketones can supply > 60% of the brain’s energy requirements, and are preferentially taken up by the brain over glucose. This occurs in cognitively normal younger and older adults, as well as in those with mild cognitive impairment (MCI) and AD.
Ketones can also be induced with a very low carbohydrate high fat (VLCHF) diet. Medium chain triglyceride (MCT) oil has the potential to produce a nutritional source of ketones for an alternative brain fuel to glucose, or by the consumption of MCT oil or esterases in freeze‐dried form. This is independent of the fasting state or carbohydrate intake. Long‐term compliance with fasting or VLCHF and LCHF diet regimes is challenging and requires strict medical supervision. Hence, the potential advantage of nutritional ketone sources (MCT) over these restrictive diets. Our recent study showed a clear dose‐dependent effect on ketone (BHB) generation with varying doses of MCT supplementation, and was found to be equivalent in young, elderly, and AD subjects.
In Alzheimer Disease (AD), the brain is unable to use glucose normally, causing hypofunction of 20% to 40% in key areas of the brain responsible for the symptoms in AD.
The MCT oil used was Bulletproof Brain Octane ® (NPN 80057199). Are other MCT oils just as good? Hell if I know. The goal dose was three tablespoons (15 ml) daily. My sense is that it was recommended as one tablespoon (15 ml) three times daily. The average consumption ended up as two tablespoons daily. Caregivers were in charge of dosing and they tended to forget or omit the lunchtime dose. Some study participants had limited dosing due to MCT side effects: abdominal pain, diarrhea, or vomiting.
Conclusion:
This study shows that participants taking MCT supplementation for 11 months continuously did better cognitively than their peers who had their 11 months of MCT interrupted by 4 months of placebo (olive) oil. Given that most patients should experience a drop in their cognitive scores over the 15 months, the fact that those on longer continuous MCT did not, could be a sample size error for the outcomes other than Montreal Cognitive Assessment, but it could also be that the difference in scores (showing stability) is valid.
In other words, MCT oil didn’t improve cognition, but stabilized it. I.e., it prevented the usual expected decline over time.
I was saddened to hear of the untimely death of Dr Sarah Hallberg even though I didn’t know her personally. DietDoctor has a tribute article about her in case you’re not familiar. An excerpt:
Dr. Hallberg first burst onto the low carb scene with a 2015 TED Talk: “Reversing type 2 diabetes starts with ignoring the guidelines” The video advocated using a low carb diet – eating minimally unprocessed whole foods like eggs, meat, and vegetables with butter or cheese – to improve blood sugar and reverse diabetes symptoms.
The video went viral and has now had more than 8.6 million views. As news of her passing spread, hundreds of viewers posted on the site saying how her advice had saved their lives.
Judicious alcohol consumption is a reasonable component of many successful ketogenic diets. But the practice can also be a dangerous minefield. Anne Mullins over at DietDoctor has a great article that will steer you away from the mines. An excerpt:
Nyström notes that alcohol is actually the fourth macronutrient after protein, fats and carbohydrates, and that in many nutrition studies its intake is often overlooked. In Mediterranean countries like Greece and Italy, alcohol makes up about 10 % of caloric intake and may partially contribute to the touted benefits of the Mediterranean diet, Nyström says.
Drinking alcohol, however, may slow weight loss for some. Dr. Sarah Hallberg advises her patients who are trying to lose weight and/or reverse diabetes to have a maximum 1 glass of wine for women and 2 for men, and not every day. “If they experience any weight stall, I recommend they stop the alcohol completely,” says Hallberg.
Both Dr. Jason Fung and Dr. Ted Naiman discourage any alcohol use among patients in their care who are still trying to lose weight, reverse diabetes or heal a fatty liver (see point 5). “I find alcohol is not conducive to steady weight loss,” says Fung.
Read the whole thing to learn about the dopamine reward system, alcohol abuse and addiction, liver diseases, and worse hangovers. If you regularly drink to the point of hangovers, that’s too much alcohol!
Steve Parker, M.D.
PS: Conquer Diabetes and Prediabetes includes a doctor-designed ketogenic diet as one option for weight loss and diabetes management.