
People with diabetes may have specific issues that need to be taken into account when exercising.
DIABETIC RETINOPATHY
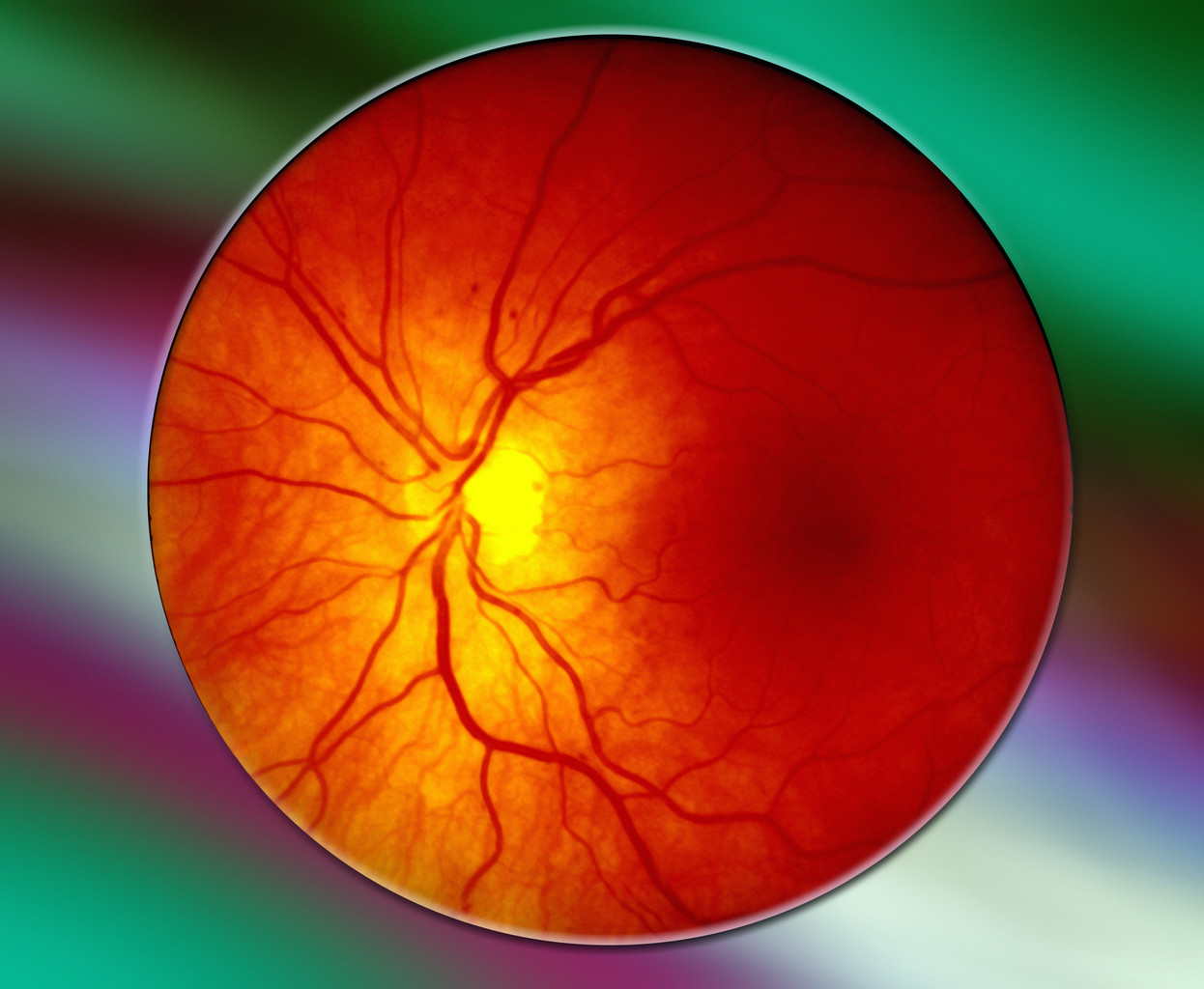
Photo of the retina at the back of the eyeball
Retinopathy, an eye disease caused by diabetes, increases risk of retinal detachment and bleeding into the eyeball called vitreous hemorrhage. These can cause blindness. Vigorous aerobic or resistance training may increase the odds of these serious eye complications. Patients with retinopathy may not be able to safely participate. If you have any degree of retinopathy, avoid the straining and breath-holding that is so often done during weightlifting or other forms of resistance exercise. Vigorous aerobic exercise may also pose a risk. By all means, check with your ophthalmologist first. You don’t want to experiment with your eyes.
DIABETIC FEET AND PERIPHERAL NEUROPATHY
Diabetics are prone to foot ulcers, infections, and ingrown toenails, especially if peripheral neuropathy (numbness or loss of sensation) is present. Proper foot care, including frequent inspection, is more important than usual if a diabetic exercises with her feet. Daily inspection should include the soles and in-between the toes, looking for blisters, redness, calluses, cracks, scrapes, or breaks in the skin. See your physician or podiatrist for any abnormalities. Proper footwear is important (for example, don’t crowd your toes). Dry feet should be treated with a moisturizer regularly. In cases of severe peripheral neuropathy, non-weight-bearing exercise (e.g., swimming or cycling) may be preferable. Discuss with your physician or podiatrist.
HYPOGLYCEMIA
Low blood sugars are a risk during exercise if you take diabetic medications in the following classes: insulins, sulfonylureas, meglitinides, and possibly thiazolidinediones and bromocriptine.
Are you sure your symptoms are from hypoglycemia?
Hypoglycemia is very uncommon with thiazolidinediones. Bromocriptine is so new (for diabetes) that we have little experience with it; hypoglycemia is probably rare or non-existent. Diabetics treated with diet alone or other medications rarely have trouble with hypoglycemia during exercise.
Always check your blood sugar before an exercise session if you are at risk for hypoglycemia. Always have glucose tablets, such as Dextrotabs, available if you are at risk for hypoglycemia. Hold off on your exercise if your blood sugar is over 200 mg/dl (11.1 mmol/l) and you don’t feel well, because exercise has the potential to raise blood sugar even further early in the course of an exercise session.
As an exercise session continues, active muscles may soak up bloodstream glucose as an energy source, leaving less circulating glucose available for other tissues such as your brain. Vigorous exercise can reduce blood sugar levels below 60 mg/dl (3.33 mmol/l), although it’s rarely a problem in non-diabetics.
The degree of glucose removal from the bloodstream by exercising muscles depends on how much muscle is working, and how hard. Vigorous exercise by several large muscles will remove more glucose. Compare a long rowing race to a slow stroll around in the neighborhood. The rower is strenuously using large muscles in the legs, arms, and back. The rower will pull much more glucose out of circulation. Of course, other metabolic processes are working to put more glucose into circulation as exercising muscles remove it. Carbohydrate consumption and diabetic medications are going to affect this balance one way or the other.
If you are at risk for hypoglycemia, check your blood sugar before your exercise session. If under 90 mg/dl (5.0 mmol/l), eat a meal or chew some glucose tablets to prevent exercise-induced hypoglycemia. Re-test your blood sugar 30–60 minutes later, before you exercise, to be sure it’s over 90 mg/dl (5.0 mmol/l). The peak effect of the glucose tablets will be 30–60 minutes later. If the exercise session is long or strenuous, you may need to chew glucose tablets every 15–30 minutes. If you don’t have glucose tablets, keep a carbohydrate source with you or nearby in case you develop hypoglycemia during exercise.
Re-check your blood sugar 30–60 minutes after exercise since it may tend to go too low.

For myself, I prefer high intensity interval training (HIIT) over long slow cardio (aerobics)
If you are at risk of hypoglycemia and performing moderately vigorous or strenuous exercise, you may need to check your blood sugar every 15–30 minutes during exercise sessions until you have established a predictable pattern. Reduce the frequency once you’re convinced that hypoglycemia won’t occur. Return to frequent blood sugar checks when your diet or exercise routine changes.
These general guidelines don’t apply across the board to each and every diabetic. Our metabolisms are all different. The best way to see what effect diet and exercise will have on your glucose levels is to monitor them with your home glucose measuring device, especially if you are new to exercise or you work out vigorously. You can pause during your exercise routine and check a glucose level, particularly if you don’t feel well. Carbohydrate or calorie restriction combined with a moderately strenuous or vigorous exercise program may necessitate a 50 percent or more reduction in your insulin, sulfonylurea, or meglitinide. Or the dosage may need to be reduced only on days of heavy workouts. Again, enlist the help of your personal physician, dietitian, diabetes nurse educator, and home glucose monitor.
Finally, insulin users should be aware that insulin injected over muscles that are about to be exercised may get faster absorption into the bloodstream. Blood sugar may then fall rapidly and too low. For example, injecting into the thigh and then going for a run may cause a more pronounced insulin effect compared to injection into the abdomen or arm.
AUTONOMIC NEUROPATHY

His heart’s on fire! (My son made this)
This issue is pretty technical and pertains to function of automatic, unconscious body functions controlled by nerves. These reflexes can be abnormal, particularly in someone who’s had diabetes for many years, and are called autonomic neuropathy. Take your heart rate, for example. It’s there all the time, you don’t have to think about it. If you run to catch a bus or climb two flights of stairs, your heart rate increases automatically to supply more blood to exercising muscles. If that automatic reflex doesn’t work properly, exercise is more dangerous, possibly leading to passing out, dizziness, and poor exercise tolerance. Other automatic nerve systems control our body temperature regulation (exercise may overheat you), stomach emptying (your blood sugar may go too low), and blood pressure (it could drop too low). Only your doctor can tell for sure if you have autonomic neuropathy.
GETTING STARTED
I’ve run out of time today. For ideas, scan some of the articles under the Exercise category in the far right panel. FYI, here’s what I’m doing, but it’s not a good place for rank beginners to start. If you want to being resistance training, strongly consider some sessions with a personal trainer.



