
I couldn’t find a decent picture of a liver or pancreas, so this will have to do….
Excessive insulin output by the pancreas (hyperinsulinemia) is the underlying cause of type 2 diabetes, according to a hypothesis from Walter Pories, M.D., and G. Lynis Dohm, Ph.D. The cause of the hyperinsulinemia is a yet-to-be-identified “diabetogenic signal” to the pancreas from the gastrointestinal tract.
This is pretty sciencey, so you’re excused if you stop reading now. You probably should.
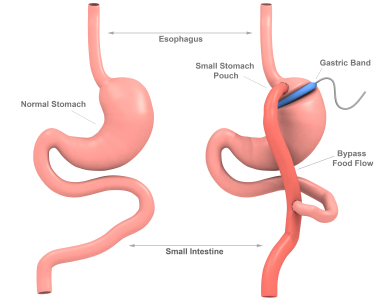
They base their hypothesis on the well-known cure or remission of many cases of type 2 diabetes quite soon after roux-en-y gastric bypass surgery (RYGB) done for weight loss. (Recent data indicate that six years after surgery, the diabetes has recurred in about a third of cases.) Elevated fasting insulin levels return to normal within a week of RYGB and remain normal for at least three months. Also soon after surgery, the pancreas recovers the ability to respond to a meal with an appropriate insulin spike. Remission or cure of type 2 diabetes after RYGB is independent of changes in weight, insulin sensitivity, or free fatty acids.
Bariatric surgery provides us with a “natural” experiment into the mechanisms behind type 2 diabetes.
The primary anatomic change with RYGB is exclusion of food from a portion of the gastrointestinal tract, which must send a signal to the pancreas resulting in lower insulin levels, according to Pories and Dohm.
Why would fasting blood sugar levels fall so soon after RYGB? To understand, you have to know that fasting glucose levels primarily reflect glucose production by the liver (gluconeogenesis). It’s regulated by insulin and other hormones. Insulin generally suppresses gluconeogenesis. The lower insulin levels after surgery should raise fasting glucose levels then, don’t you think? But that’s not the case.
Pories and Dohm surmise that correction of hyperinsulinemia after surgery leads to fewer glucose building blocks (pyruvate, alanine, and especially lactate) delivered from muscles to the liver for glucose production. Their explanation involves an upregulated Cori cycle, etc. It’s pretty boring and difficult to follow unless you’re a biochemist.
The theory we’re talking about is contrary to the leading theory that insulin resistance causes hyperinsulinemia. Our guys are suggesting it’s the other way around: hyperinsulinemia causes insulin resistance. It’s a chicken or the egg sort of thing.
If they’re right, Pories and Dohm say we need to rethink the idea of treating type 2 diabetes with insulin except in the very late stages when there may be no alternative. (I would add my concern about using insulin secretagogues (e.g., sulfonylureas) in that case also.) If high insulin levels are the culprit, you don’t want to add to them.
We’d also need to figure out what is the source of the “diabetogenic signal” from the gastrointestinal tract to the pancreas that causes hyperinsulinemia. A number of stomach and intestinal hormones can affect insulin production by the pancreas; these were not mentioned specifically by Pories and Dohm. Examples are GIP and GLP-1 (glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1).
Keep these ideas in mind when you come across someone who’s cocksure that they know the cause of type 2 diabetes.
Steve Parker, M.D.
Reference: Pories, Walter and Dohm, G. Lynis. Diabetes: Have we got it all wrong? Hyperinsulinism as the culprit: surgery provides the evidence. Diabetes Care, 2012, vol. 35, p. 2438-2442.

![MP900308894[1]](https://diabeticmediterraneandiet.com/wp-content/uploads/2012/02/mp9003088941.jpg)



