Knees are the most common joint affected by osteoarthritis. Photo credit: Steven Paul Parker II
Have you heard of the “diabetic triad”? Diabetes (type 2) + hypertension + arthritis. Very common.
A MedPage Today article indicates that chronic stress may precipitate or aggravate arthritis. Even childhood stress. The link is not as strong for rheumatoid arthritis as it is for more common types of arthritis. Most for the reviewed studies “categorized stress as stemming from adverse life events … or adverse childhood experiences …. Most studies … suggested a relationship between exposure to chronic stressors and arthritis development.”
Would stress reduction improve the quality of life of arthritis patients? The study at hand doesn’t address that but I’d wager that it does.
A couple of dietitians did an massive literature review looking for evidence that diet has an effect on major health conditions such as obesity, diabetes, and cardiovascular disease. Sounds interesting, and similar to my own obsessive review done between 1995 and 2005. It bothers me that “hypertension” is misspelled in the abstract. For the researchers’ conclusions, you have to pay $27.95 USD.
Appropriate diet can prevent, manage, or reverse noncommunicable health conditions such as obesity, cardiovascular disease, and diabetes. Consequently, the public’s interest in diet and nutrition has fueled the multi-billion-dollar weight loss industry and elevated its standing on social media and the internet. Although many dietary approaches are popular, their universal effectiveness and risks across overall populations are not clear. The objective of this scoping review was to identify and characterize systematic reviews (SRs) examining diet or fasting (intermittent energy restriction [IER]) interventions among adults who are healthy or may have chronic disease. An in-depth literature search of six databases was conducted for SRs published between January 2010 and February 2020. A total of 22,385 SRs were retrieved, and 1,017 full-text articles were screened for eligibility. Of these, 92 SRs met inclusion criteria. Covered diets were organized into 12 categories: high/restricted carbohydrate (n = 30), Mediterranean, Nordic, and Tibetan (n = 19), restricted or modified fat (n = 17), various vegetarian diets (n = 16), glycemic index (n = 13), high protein (n = 12), IER (n = 11), meal replacements (n = 11), paleolithic (n = 8), Dietary Approaches to Stop Hypretension (DASH; n = 6), Atkins, South Beach, and Zone (n = 5), and eight other brand diets (n = 4). Intermediate outcomes, such as body weight or composition and cardiometabolic, were commonly reported. Abundant evidence was found exploring dietary approaches in the general population. However, heterogeneity of diet definitions, focus on single macronutrients, and infrequent macronutrient subanalyses were observed. Based on this scoping review, the Evidence Analysis Center prioritized the need to collate evidence related to macronutrient modification, specifically restricted carbohydrate diets.
These are the ones I take. In the U.S., your best price may be at Costco or Sam’s Club.
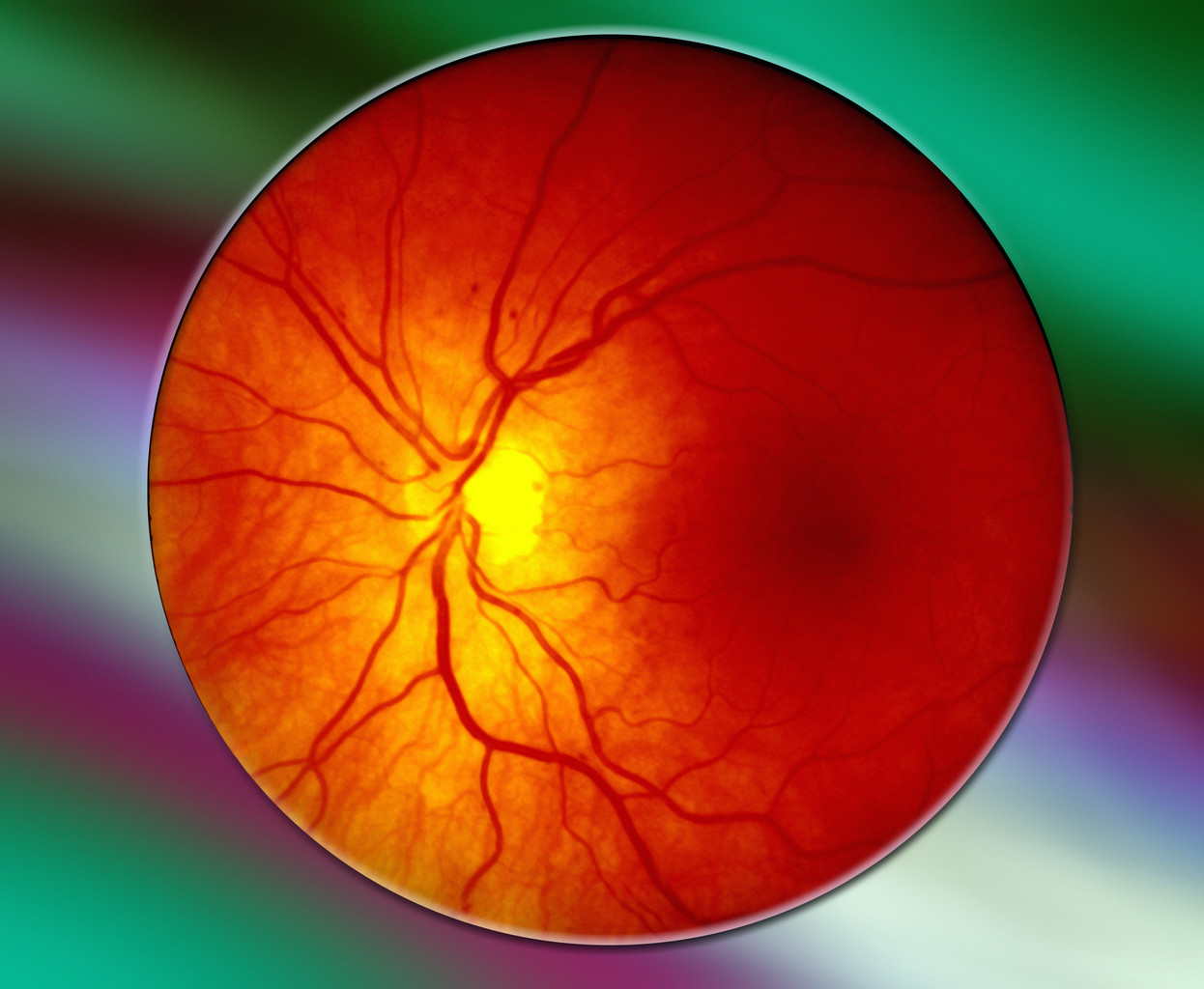
I have a particular interest in preventing age-related macular degeneration (ARMD) since it runs in my family. It’s the leading cause of vision loss in adults over 50.
Question What were the long-term findings of Age-Related Eye Disease Study 2 (AREDS2) supplements regarding development of lung cancer or progression to late age-related macular degeneration (AMD)?
Findings In this epidemiologic follow-up study of the AREDS2 cohort of 3882 participants and 6351 eyes, 10-year follow-up results showed that development of lung cancer nearly doubled in participants assigned to beta carotene among former smokers but not those assigned to lutein/zeaxanthin. Lutein/zeaxanthin was associated with a reduction in the risk of progression to late AMD when compared with beta carotene.
Meaning These findings suggest that the AREDS2 supplement with lutein/zeaxanthin instead of beta carotene was safe, with no association with developing lung cancer and a potential beneficial association with further reduction in progression to late AMD.
…. 10-year weight gain is substantially greater in US women compared to men. On average (±SE), women gained 5.4 ± 0.3 kg and 9.2 ± 0.4 percent of their initial weight over the previous 10 years, whereas men gained 2.6 ± 0.2 kg and 3.8 ± 0.3 percent of their initial weight. In general, compared to US men, women gained about twice as much weight (kg) and 2.4 times more weight expressed as a percent of initial weight, over the previous 10 years. Fourth, 10-year weight gain is significantly higher in Non-Hispanic Blacks than in other racial groups, especially NH [non-Hispanic] Black women. Moreover, 10-year weight gain is significantly lower in Non-Hispanic Asians compared to other racial categories.
If you think in pounds instead of kilograms, like me, note that 1 kg = 2.2 lb.
Since 2000, U.S. obesity in adults has increased from 30% to 42% of the population. This doesn’t even include suspected pandemic-related weight gain.
Mean [~average] 10-year weight gain was 4.2 ± 0.2 kg or 6.6 ± 0.2% of initial body weight within the United States.
The incidence of severe obesity had increased from 5% in 2000 to almost 10% now. (The article likely defines “severe obesity” but I didn’t catch it in my quick scan.)
Not enough Americans are reading and implementing my books!
The Mediterranean diet is constantly lauded in the nutrition world—in fact, U.S. News has named it the “best diet overall” for five years straight—but as a registered dietitian, I think it’s time to think about it a little differently: It’s time to dethrone the Mediterranean diet as being the very best way to eat.
Now, the Mediterranean diet—which emphasizes whole grains and plant foods such as fruits, vegetables, legumes, tree nuts, seeds, and olives, and limits red meat, sugar, and saturated fat—is not the only culturally based way of eating that’s been celebrated. The Japanese diet, rich in foods such as seafood, steamed rice, tofu, natto, seaweed, and pickled fruits and vegetables, has been promoted for its longevity-promoting aspects as well. But as scrolling through social media or even many news and health websites will show, it still doesn’t come close to the Mediterranean diet in terms of widespread recognition.
As an RD, I’ve noticed an overwhelming belief in our society that eating Mediterranean-style is just the way to go. So if your cultural foods don’t hail from one of the countries that make up that area, how does this make you feel?
Spoiler: Probably not so good—and that’s why I believe we need to rethink how we talk about cultural foods and ways of eating.
You know I’m a Mediterranean diet advocate. There are other healthy ways of eating. I’m an advocate of free speech and open debate. No censorship here! Read it and see what you think. I’m not sure what the “Japanese diet” is. I’ve written good things about the Okinawan diet as discussed in Dan Buettner’s Blue Zones books. Click for my review of Blue Zones.
At baseline, the mean body weight was 104.8 kg, the mean BMI was 38.0, and 94.5% of participants had a BMI of 30 or higher. The mean percentage change in weight at week 72 was −15.0% (95% confidence interval [CI], −15.9 to −14.2) with 5-mg weekly doses of tirzepatide, −19.5% (95% CI, −20.4 to −18.5) with 10-mg doses, and −20.9% (95% CI, −21.8 to −19.9) with 15-mg doses and −3.1% (95% CI, −4.3 to −1.9) with placebo (P<0.001 for all comparisons with placebo). The percentage of participants who had weight reduction of 5% or more was 85% (95% CI, 82 to 89), 89% (95% CI, 86 to 92), and 91% (95% CI, 88 to 94) with 5 mg, 10 mg, and 15 mg of tirzepatide, respectively, and 35% (95% CI, 30 to 39) with placebo; 50% (95% CI, 46 to 54) and 57% (95% CI, 53 to 61) of participants in the 10-mg and 15-mg groups had a reduction in body weight of 20% or more, as compared with 3% (95% CI, 1 to 5) in the placebo group (P<0.001 for all comparisons with placebo).
Three to 7% of users stopped the drug due to side effects.
Nutritional discipline and dietary restriction result in resistance exercise for our cells. Triggered by calorie restriction or physical exercise, our cells end up producing transcription factors that lead to protection against oxidation, inflammation, atherosclerosis, and carcinogenic proliferation. In the long-term, this results in longevity and a decrease in cancer, T2DM [type 2 diabetes], myocardial infarction, and stroke. Since centuries past, studies on humans, rhesus monkeys, and multilevel organisms have demonstrated the benefits of calorie restriction without malnutrition. Periodic fasting and calorie restriction show increases in regeneration markers and decreases in biomarkers for diabetes, CVD [cardiovascular disease], cancer, and aging.
The present review concluded that longevity can be increased through moderation of diet and exercise. Research shows that a concoction of the diverse diets modernly popularized— MED [Mediterranean], DASH, high-protein diets±—tempered by overall calorie restriction through periodic fasting or chronic calorie restriction, will provide protection against CVD, cancer, and aging. Exercise has also been shown to increase longevity in the general population, lower incidence of diabetes and cancer, and produce psychological benefits.
This review of research indicates that incorporating a moderate caloric restriction or fasting regimen could provide substantial benefits at low risk. Cellular exercise through calorie restriction and physical exercise can increase longevity and prevent the greatest killers of human society today—stroke and heart disease.
I have posted one or more cabbage recipes on this blog. Use the search box if interested.
When I was a wee lad, my mother never served cabbage. Don’t know why.
Adam Piggott is a good writer. He claims he has the best cabbage recipe ever. Here ’tis:
Ingredients:
1 fresh green cabbage
Salt
Cumin
Apple [cider] vinegar
Extra virgin olive oil.
Remove the rough outside leaves of the cabbage and then cut it into quarters. Using a mandoline slicer or a grater, carefully shave the cabbage as thinly as possible.
Now add the other ingredients in the order in which I listed them. Then mix well together and leave to sit for a few hours. Yes, a few hours and the longer the better. A minimum of one hour but if you can leave it all afternoon then you will thank me. This is why I was worried about them running out at the lunch. The cabbage will release some fluids over this time. Check for seasoning and olive oil before serving as you may have to add a little more.
His original post didn’t include specific amounts of most ingredients. Adam elaborated in the comments section:
Yes, the amounts are the issue here and it is what makes this a unique dish. Salt is the key. I use a large salt grinder which you can see in the last photo. I had half a cabbage for lunch and I would say that I used a good half tablespoon of salt. I added a little more at the end. Remember though with salt – you can always add more but you can’t take any away.
I used a quarter teaspoon of cumin. You’re just after a hint of the taste there. A small splash of the vinegar. Too much vinegar becomes overpowering; you can always add more later if you think you need it. Olive oil you can give it a good splash. Looking at the bowl of cabbage you should not see any liquid oozing out of the bottom. If you do then you have used too much oil or vinegar.
You can definitely refrigerate it but you don’t have to. If you do then you should cover it with cling film.